
-
Basics of ECG Interpretation11 Topics
-
Normal ECG Parameters
-
ECG Interpretation of Chamber Enlargement4 Topics
-
Dysrhythmias
-
Bradycardia
-
Heart Block3 Topics
-
Sick Sinus Syndrome
-
Tachycardia8 Topics
-
Hyperkalemia
-
Myocardial Hypoxia/Ischemia
-
Low Amplitude QRS Complex
-
Wide QRS Complex
-
Bundle Branch Block
-
Differentials for ECG Abnormalities
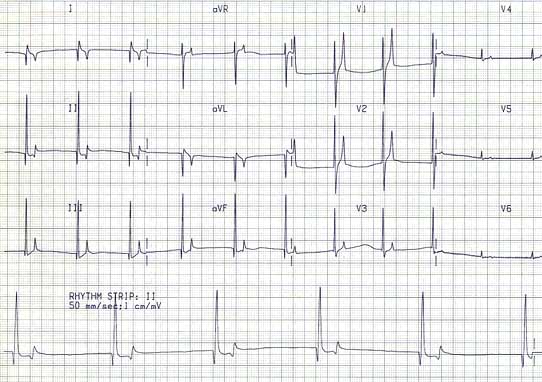
Hyperkalemia results in:
- Inhibition of atrial myocardial depolarization
- Slowing of heart rate
- Prolongation of QRS depolarization
- And may result in ventricular fibrillation or asystole when very severe
The ECG is a poor substitute for serum potassium levels to determine the degree of abnormality.
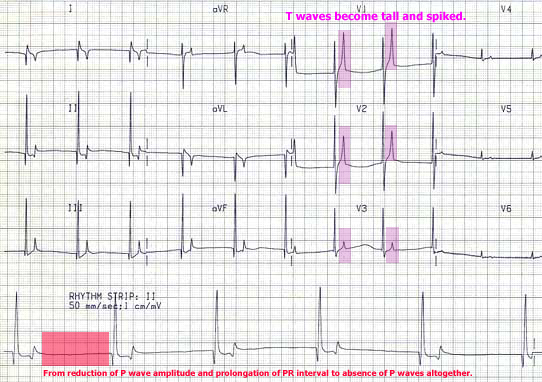
ECG Findings:
- From reduction of P wave amplitude and prolongation of PR interval to absence of P waves altogether
- Increase in QRS duration
- Increase of QT duration
- Slowing of heart rate
- T waves become tall and spiked
- Decreased R wave amplitude
Etiology:
- Addison’s Disease (hypoadrenocorticism)
- Obstructive urinary disease
- Oliguric, anuric renal disease
- Acidosis
- Uncontrolled diabetic ketoacidosis
Treatment:
- IV fluids, using 0.9% NaCl (if no urinary obstruction)
- Sodium bicarbonate to correct acidosis
- Calcium gluconate antagonizes the cardiotoxic effects of potassium
- IV glucose and insulin may be needed to drive potassium intracellularly
- Treat the underlying disease
Prognosis: Excellent response to prompt therapy
Comments:
- This disorder must be distinguished from atrial standstill or silent atrium, a diffuse atrial myocardial disorder wherein the atrial tissue is neither capable of initiating an impulse nor being activated (also known as atrioventricular muscular dystrophy). This disorder will not respond to potassium reductive therapy.
- The most specific ECG feature is the absence of P waves. At times these may be difficult to identify in the frontal plane leads. The V leads are usually the best leads to illustrate P waves.