
-
Basics of ECG Interpretation11 Topics
-
Normal ECG Parameters
-
ECG Interpretation of Chamber Enlargement4 Topics
-
Dysrhythmias
-
Bradycardia
-
Heart Block3 Topics
-
Sick Sinus Syndrome
-
Tachycardia8 Topics
-
Hyperkalemia
-
Myocardial Hypoxia/Ischemia
-
Low Amplitude QRS Complex
-
Wide QRS Complex
-
Bundle Branch Block
-
Differentials for ECG Abnormalities
Lesson Progress
0% Complete
Due to failure of the sino-atrial impulse to activate the ventricular myocardium after activating the atrial myocardium.
Depending on the location of the abnormality it may be classified as:
- Mobitz type 1 (Wenckebach)
- Mobitz type 2
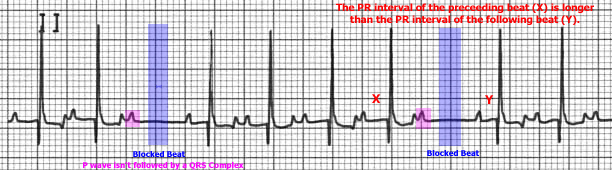
Mobitz type 1 (Wenckebach) Second Degree Heart Block:
ECG Findings:
- P wave that is not followed by a QRS complex
- QRS complex is usually of normal duration and morphology
- The PR interval progressively prolongs just prior to the blocked beat
- When comparing the PR interval of the beat immediately preceding the blocked beat with that of the beat immediately following the blocked beat, the PR interval of the preceding beat is longer than the PR interval of the following beat.

Etiology:
- Due to failure of the sino-atrial impulse to propagate through the AV node
- Excessive vagal tone can cause this abnormality
- May be normal in some dogs
- Drug therapy (e.g. digitalis, beta blocker, calcium channel blocker)
Consequences:
- Very rarely is the heart rate sufficiently reduced to cause any reduction in cardiac output, so it is often not clinically significant.
- This rhythm disturbance is important to distinguish from second degree heart block of the Mobitz type 2 variety which is often more clinically significant.
Treatment:
- Often none required
- Often atropine responsive
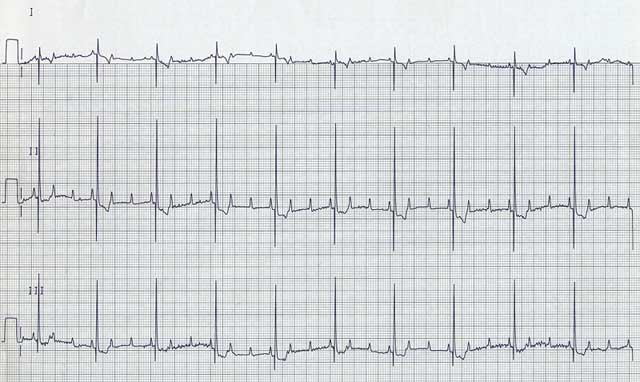
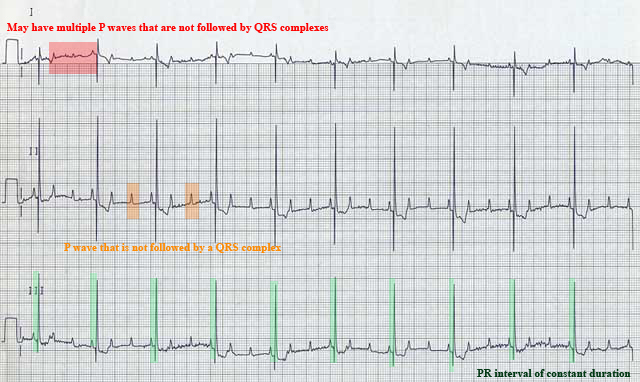
Mobitz Type 2 Second Degree Heart Block:
ECG Findings:
- P wave that is not followed by a QRS complex
- May have a wide QRS complex (not in example shown)
- PR interval of constant duration for the QRS present
- May have multiple P waves that are not followed by QRS complexes (i.e. 2:1, 3:1, 4:1, etc. block)
Etiology:
- Due to failure of the sino-atrial impulse to propagate through the AV node, His bundle, or bundle branches
- Associated with organic disease of the His bundle or bundle branches. This may be in the form of an ischemic area, scar/fibrosis, inflammation, infection with necrosis, neoplasia or granuloma
Consequences:
- Evidence of reduced cardiac output may occur if the ventricular rate is substantially reduced and depending on their activity
- May progress to 3rd degree (complete) heart block (see below)
Treatment:
- Usually not responsive to atropine or glycopyrrolate
- The ventricular rate can usually be increased with intravenous isoproterenol
- Unless the ventricular rate is slow and clinical signs present, no treatment may be required
- Permanent pacemaker implantation may be indicated in some cases